For Tecla Bhamu, malaria no longer arrives as an emergency.
It arrives as a season.
The first time, her husband collapsed with fever and convulsions in their Hurungwe village after days of vomiting and chills.
With no ambulance available and roads damaged by heavy rains, neighbours loaded him onto a scotch cart and pushed him for kilometres to Chitindiva Clinic.
Weeks later, malaria struck again.
This time it was her daughter.
By the time the child reached Karoi District Hospital, she could barely stand.
- Malaria fight disrupted by COVID pandemic: WHO
- Malaria fight disrupted by COVID pandemic: WHO
- Co-operate to curb malaria, Mash West farmers urged
- Vaccines could be a game-changer in the fight against malaria in Africa
Keep Reading
Each illness brought new costs — transport money, food expenses, lost farming time and medicine shortages.
“We now expect malaria every rainy season,” Bhamu said quietly. “It keeps coming back.”
Across Mashonaland West province as well as northern and eastern parts of Zimbabwe, malaria is resurging at alarming speed as the country’s frontline prevention systems weaken following major international aid cuts, shrinking mosquito net supplies and overstretched rural healthcare services.
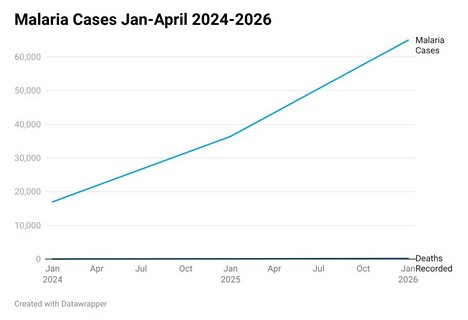
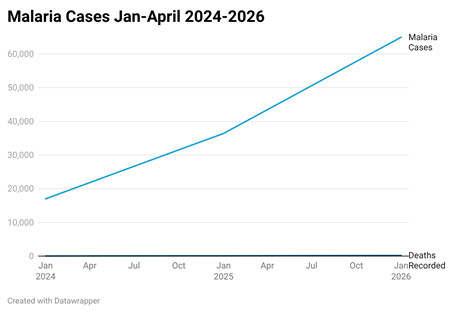
By mid-April this year, Zimbabwe had recorded more than 65 000 malaria infections and 174 deaths — a dramatic increase from nearly 17 000 infections and 34 deaths recorded during the same period in 2024.
A month-long investigation carried by Standard People reveal that the outbreak is exposing how heavily Zimbabwe’s malaria response depended on foreign-funded systems that are now crumpling faster than authorities can replace them.
For years, donor-backed programmes quietly financed much of the country’s malaria infrastructure, including mosquito net procurement, indoor spraying campaigns, rapid testing kits, disease surveillance systems and village health workers operating in remote communities.
However, after sweeping cuts to United States foreign aid programmes in 2025, many malaria intervention programmes shrunk, Standard People established.
One of the country’s largest malaria initiatives, the Zimbabwe Assistance Programme in Malaria (Zapim), was terminated after years of supporting prevention and treatment systems across high-risk districts.
Health and Child Care ministry officials, who spoke on conditions of anonymity, concede the consequences are now becoming visible in overwhelmed clinics, rising infections and communities increasingly left without protection during peak mosquito breeding seasons.
Prevention systems on the brink
Zimbabwe’s malaria response had once been regarded as one of the country’s major public health success stories.
Between 2006 and 2015, infections declined significantly following aggressive prevention campaigns funded largely through international donor support.
Mosquito net distribution expanded nationwide, indoor residual spraying intensified and village health workers strengthened disease surveillance in vulnerable rural communities.
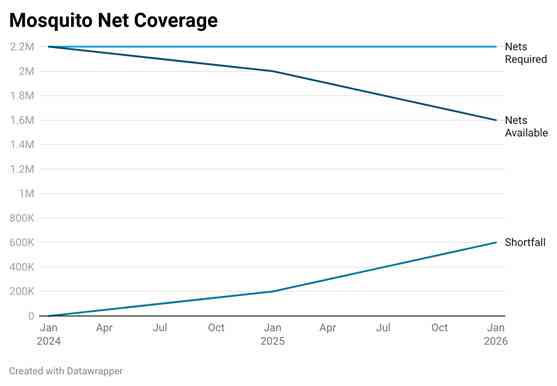
Health and Child Care ministry data show that the shutdown of Zapim alone created a shortfall of more than 600 000 insecticide-treated mosquito nets that had been expected to protect vulnerable households across the country.
In some communicated visited by Standard People, villagers say indoor residual spraying campaigns were delayed or scaled down.
Several rural communities are also losing access to frontline village health workers who previously monitored outbreaks, promoted prevention and encouraged early treatment.
Public health expert Johannes Marisa warned that weakened prevention systems almost always trigger rapid increases in infections.
“When prevention systems weaken, the first thing you see is rising infections,” Marisa said.
“Deaths follow when health facilities become overwhelmed or people fail to access treatment in time.”
Although international agencies financed much of the country’s malaria infrastructure for years, investigations by Standard People revealed government’s failure to develop strong contingency plans once foreign support began shrinking.
“Mosquito net procurement, spraying campaigns and surveillance systems are all in shambles and in most districts, the annual indoor residual spraying was not done coupled by insecticide-treated mosquito nets shortages,” said an insider within the Health and Child Care ministry.
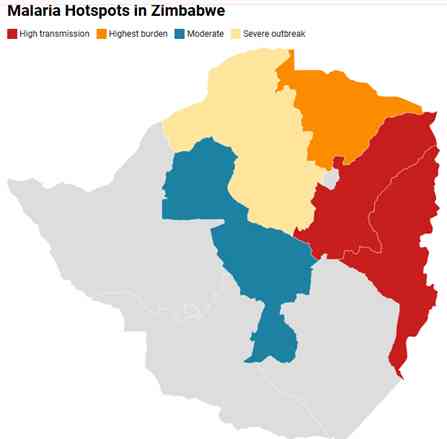
Hotspots spreading across northern Zimbabwe
While Mashonaland West has emerged as one of the country’s hardest-hit provinces, outbreaks are spreading aggressively across northern and eastern Zimbabwe.
Data from the Health and Child Care ministry show that Mashonaland Central recorded nearly 50 000 infections, almost 40% of national malaria cases, while Manicaland contributed more than 27 000 infections.
Mashonaland East has also experienced rising transmission linked to prolonged rainfall and weakened prevention systems.
Although Mashonaland West recorded fewer infections than Mashonaland Central, its death burden has remained disproportionately high.
Data from the International Federation of Red Cross and Red Crescent Societies show that Mashonaland West province recorded 11 790 infections and 76 deaths, raising concerns over delayed treatment, poor clinic accessibility and fragile rural healthcare systems.
Malaria incidence in Mashonaland West increased sharply from 1.54 per 1,000 population between weeks one and 18 in 2024 to 7.66 per 1,000 during the same period in 2025, nearly a fivefold increase.
Districts such as Hurungwe, Kariba, Makonde and Sanyati have emerged as major transmission hotspots.
Health and Child Care officials said infections are spreading fastest in areas with high rainfall, flood-damaged roads and weakened prevention coverage.
Rural clinics pushed beyond capacity
In many districts, rising malaria infections are colliding with fragile healthcare systems already struggling with staff shortages, medicine gaps and transport breakdowns.
Mashonaland West operates one provincial hospital, 21 hospitals and more than 190 clinics spread across government, mission and private ownership.
Standard People established that in many rural communities in Mashonaland West province, patients travel between five and 10 kilometres to reach the nearest clinic, often relying on scotch carts, bicycles or informal transport during the rainy season.
National malaria treatment guidelines require patients to receive treatment within 24 hours of symptom onset to prevent severe complications.
However, village health workers in Hurungwe and Nyaminyami say many patients arrive too late at health centres.
“Many people first rely on home remedies before coming to clinics,” one village health worker said.
“By the time some patients arrive, they are already very weak.”
A visit to a number of clinics in Hurungwe and Makonde districts show that that some clinics periodically run short of rapid malaria testing kits and anti-malarial medicines during peak transmission periods.
“At some point we had shortages of Artemether/Lumefantrine, one of our primary anti-malaria treatments, including paediatric medication for children,” said a health official at a clinic in Hurungwe.
Health workers said at overstretched rural clinics, including Tengwe, Nyamakate, Vuti and Chiroti, among others, nurses are sometimes forced to attend to a number of malaria patients during peak outbreaks.
“Under such pressure, patient monitoring, emergency response and rapid diagnosis become increasingly difficult,” said a nurse at one of the clinics.
“The malaria outbreak is also exposing major weaknesses in disease surveillance systems.”
In remote farming and gold-panning communities as well as in areas along the Zambezi lowveld, malaria infections frequently go unrecorded because nearby testing and reporting centres are unavailable.
The Mola community in Nyaminyami district has only a handful of clinics, including one operated at the Ume Crocodile Farm, leaving malaria patients with limited access to healthcare during outbreaks.
Severe malaria cases often require urgent referral to Kariba District Hospital, nearly 100 kilometres away across rugged and poorly maintained roads.
“During the rainy season, travel becomes even more difficult as flooding and damaged roads delay transport,” said a humanitarian worker operating in the area.
“For many families, the high cost of transport makes early treatment inaccessible, increasing the risk of severe illness and malaria-related deaths.”
He said the situation has worsened sharply since donor-funded malaria programmes began shrinking following international aid cuts in 2025.
“Programmes that previously supplied mosquito nets, supported village health workers and strengthened outbreak surveillance have either been scaled back or terminated, exposing already vulnerable communities such as Mola to rising infections with fewer protections in place,” he said.
“The gains are being reversed”
Save the Children country director for Zimbabwe and Malawi, Bhekimpilo Khanye in a statement said the withdrawal of donor funding had reversed years of progress achieved through joint efforts between government, aid agencies and communities.
“These projects were focused on eliminating malaria from certain regions,” Khanye said.
“When malaria parasite levels begin to fall in a community, the effect becomes cumulative because there are fewer breeding grounds and fewer infections.
“But when interventions stop, the opposite happens. Cases begin rising rapidly again.
“We are now seeing a complete reversal of the gains that had been achieved.”
Health ministry officials could not be reached for comment, but government sources said authorities have intensified vector control measures in Mashonaland West, including biolarvicides, indoor spraying campaigns and mosquito net distribution.
Zimbabwe remains highly vulnerable to malaria because nearly 67,5% of the population lives in malaria-risk areas, particularly in rural provinces.
Unlike neighbouring countries such as Botswana and South Africa — which made significant progress towards malaria elimination through sustained domestic investment and long-term prevention systems — Zimbabwe remains heavily dependent on donor-funded interventions.
For families like Bhamu’s, the consequences are already unfolding inside homes, clinics and villages across Mashonaland West province.